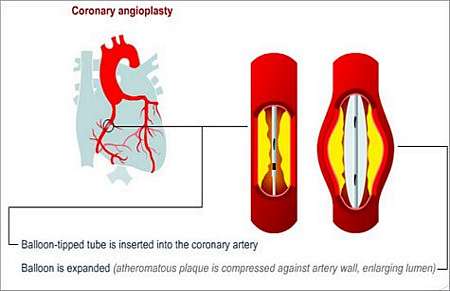
What is ANGIOPLASTY?
Angioplasty means moulding or changing the shape of a blood vessel. During this procedure, the size of an artery is increased by inflating a balloon in the artery at the site of narrowing.
This is most commonly performed in the coronary arteries, but may also be done in other blood vessels such as those supplying blood to the
- Kidneys
- Legs (femoral arteries), and
- Brain (carotid arteries)
How is this done?
- A cardiac catheterisation is performed
- Once the catheter is in the coronary artery as it arises from the aorta, a very thin wire is passed from the leg across the narrowed part of the coronary artery
- A thin tube that has a tiny balloon mounted at its tip is then fed over this wire and thereby guided to the area of narrowing in the coronary artery
- The doctor then inflates the balloon with dye using a hand-held device
- The inflated balloon can then be seen on the X-ray screen
- After about 20 seconds, the balloon in deflated and dye is once more injected down the coronary to assess the results
- Several inflations may be required to achieve a satisfactory result
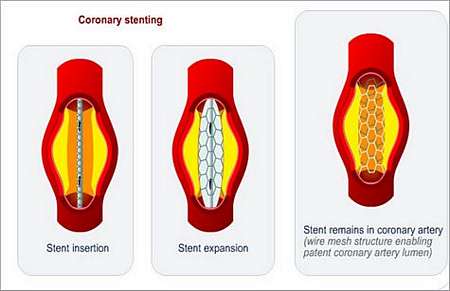
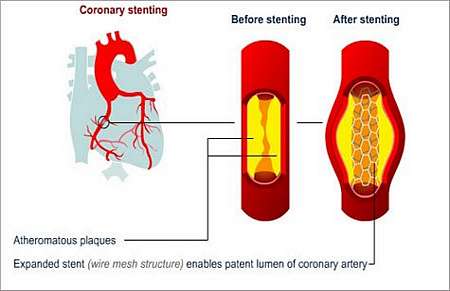
- After dilating the artery, especially with a less than optimal result, a wire mesh structure (stent) is placed at the narrowed area and expanded into the open position (this is possible because the stent is mounted over a balloon at the tip of a thin plastic tube)
- With the wire placed across the narrowed area, the stent and balloon are positioned at the narrowing and the stent is opened up as for balloon angioplasty
- Once the doctor is satisfied with the result, the catheters are removed and the patient is returned to an intensive care unit for observation
- Most patients are sent home the following day
Why is it not possible to perform angioplasty in all patients?
The presence of calcium in the wall of the artery precludes successful angioplasty.
Technical limitations such as the inability to cross the narrowed area with the wire and/or balloon.
There are certain situations where a bypass operation is a better treatment option e.g. patients with extensive disease, or high-risk patients who could not tolerate the consequences of abrupt closure of the artery, should the angioplasty not give the desired results.
The most common complications of angioplasty
- Tearing the inner lining of the vessel wall (dissection); this is very unfortunate and is treated by placing a stent over the torn area
- Unsatisfactory opening of the artery (this may be improved by using a stent)
- Acute closure of the artery causing a heart attack, or in rare instances, death (with current technology, it is possible to reopen the vessel and perhaps prevent the heart attack)
- In the 6 months following the angioplasty, the artery may become re-stenosed (narrow again) at the area of dilatation (this may be treated with a repeat angioplasty, or placement of a stent)
Follow-up after coronary angioplasty
- Patients should return for an exercise test in the month following angioplasty
- Risk factors such as hypertension, high cholesterol and diabetes need to be managed
- Patients should stop smoking
- If a stent is used at the time of angioplasty, patients need to take medication (clopidogrel) for about 3 weeks to prevent clotting of the stent
- Any chest pain experienced after the angioplasty should be taken seriously and evaluated by the treating heart specialist
© 2003 Prometheus™ Healthcare (Pty) Ltd
|